
- Reference Number: HEY1640/2026
- Departments: Ophthalmology Department
- Last Updated: 30 April 2026
Introduction
This leaflet has been produced to give you general information about your procedure. Most of your questions should be answered by this leaflet. It is not intended to replace the discussion between you and your doctor but may act as a starting point for discussion. If after reading it you have any concerns or require further explanation, please discuss this with a member of the healthcare team caring for you.
What is Keratoconus & Corneal Crosslinking (CXL)?
You have probably been troubled by some symptoms. Following discussion with your doctor they have identified a keratoconus and advised a corneal Crosslinking operation.
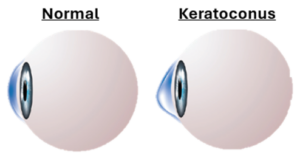
Keratoconus is a condition where the cornea weakens and bulges into a cone-like shape. This changes the way light enters the eye, causing blurred or distorted vision and increased short-sightedness. Corneal collagen crosslinking is a treatment to prevent your keratoconus getting worse by making the cornea stiffer. It is not intended to improve vision, although some patients notice minor improvements. Without treatment, the shape of the cornea can continue to worsen meaning you would eventually need a corneal transplant. By performing CXL at the correct time, a transplant could be avoided in future.
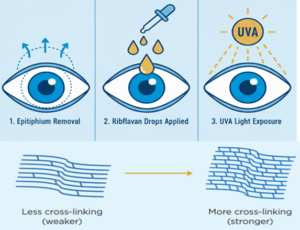
A combination of riboflavin (vitamin B2) drops, and ultraviolet (UV) light are used to form extra connections (crosslinks) between collagen fibres in the cornea. This results in your cornea becoming stronger and is also a normal part of the ageing process.
What is the Cornea?
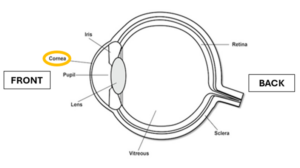
The cornea is the clear dome shaped surface at the front of your eye. It helps focus light so you can see clearly. If it becomes scarred, swollen or losses its clarity, vision becomes blurry or distorted.
Why do I need Corneal Collagen Crosslinking (CXL)?
CXL is advised if keratoconus is getting worse. This is shown by changes in your corneal scans and eye examinations. Without treatment, keratoconus can continue to worsen and affect vision. In the past, around 10 to 20% of people with keratoconus eventually needed a corneal transplant.
Your doctor will consider factors such as your age, corneal thickness, vision, and corneal shape before recommending CXL. In rare cases, the procedure may also be used if the cornea becomes weaker after laser eye surgery.
Can there be any complications or risks?
CXL is generally a safe procedure. However, as with any surgical treatment, there are possible complications and risks that must be considered carefully:
Around 3% of patients (3 in 100) may experience some vision loss after CXL due to scarring, haze, infection, or changes in corneal shape. In most cases, vision can be improved with further treatment, including corneal transplant. Higher individual risks will be discussed with you in clinic.
About 1 in 5 patients with progressive keratoconus may eventually need a corneal transplant without CXL, with the risk likely higher if treatment is not performed.
Other complications and risks will be discussed in clinic and included in the consent form prior to your operation. These may include:
- Infection
- scarring or haze
- delayed healing
- dry eye
- irregular corneal shape
- treatment failure (needing repeat CXL)
- vision changes
- possible need for corneal transplant
How do I prepare for Corneal Collagen Crosslinking (CXL)?
Please read the information leaflet. Share the information it contains with your family (if you wish) so that they can be of help and support. There may be information they need to know, especially if they are taking care of you following this examination.
The vast majority of CXL treatments are done under local anaesthetic (i.e. you will be awake). Please ensure you arrange for a friend or relative to drive you home after the procedure. Please bring a pair of sunglasses to wear after the treatment. They will help keep the eye more comfortable on the way home.
What will happen?
Your treatment will take place in the Ophthalmic Theatres on the first floor of the Eye Hospital. You should report to the Ophthalmic Day Case Unit at the time given on your patient letter. Our nursing staff will greet you. They will check your details, check your blood pressure and get you ready for surgery.
The doctor will see you before the surgery giving you the opportunity to ask any other questions you have. The doctor will use a surgical marking pen to draw an arrow over the eye we are planning to treat. When theatres are ready for you, a member of the team will collect you and walk you to theatre. Relatives may not enter the treatment room, but they can wait nearby and assist after the procedure.
Overall, the procedure takes approximately 35 minutes. At the end of the procedure, the eye doctor puts in a soft contact lens that stays in until you see the doctor in clinic. If it falls out before the clinic appointment, please throw it away. Do not try to put it back in.
The nursing staff on the day unit will run through some basic do and don’ts and discharge you with the necessary medications. You are given four types of eye drops and a short course of painkiller tablets.
What actually takes place during the CXL?
- A clip is used to keep your eyelids open and outer corneal layer (epithelium) is gently removed.
- Riboflavin drops are applied to the cornea for 30 minutes.
- UV light is shone onto the cornea for 10 minutes while riboflavin continues to be applied.
- A soft bandage contact lens is placed at the end of the procedure.
- Eye drops (steroid, antibiotic, lubricating) are provided for home use.
What happens afterwards?
Once you have been discharged you should return straight home. After the local anaesthetic used by the eye doctors has worn off, the eye can become very painful. This is normal in the first 48 hours. The eye should become progressively less painful during the first 72 hours.
We advise you rest in a darkened environment with your eyes closed. It often helps to listen to music or an audiobook to distract you from the discomfort. By day three after the operation the eye should be less painful. Once the surface of your eye has grown back over, you should be pain free. This is normally by days 5 to 7. If your eye becomes painful again after previously being pain free, you must contact the eye service immediately and arrangements will be made for you to see an eye doctor the same day.
Use your eye drops as prescribed. An appointment will be made for you in the corneal clinic. This is normally two or three days post treatment. It is likely that your doctor at this appointment will remove your bandage contact lens.
It normally takes about 2 weeks for your vision to recover back to the level of vision you had before the treatment. After your initial post-operative check-up, a further appointment is made for you for three months later. This is to check the shape of your eye and your spectacle prescription.
Possible Complications / When to seek help
Contact your ophthalmology team immediately if you notice:
- Increasing pain after 3 days
- Sudden vision loss
- Eye redness, swelling, or discharge
- Injury to the treated eye
- Bandage lens falls out
Should you require further advice on the issues contained in this leaflet, please do not hesitate to contact the Ophthalmology Department Monday to Friday 08:30AM to 18:00PM on Tel: 01482 608788 / Tel: 01482 816658 or Tel: 01482 604385 if out of hours.
General Advice and Consent
Most of your questions should have been answered by this leaflet, but remember that this is only a starting point for discussion with the healthcare team.
Consent to treatment
Before any doctor, nurse or therapist examines or treats you, they must seek your consent or permission. In order to make a decision, you need to have information from health professionals about the treatment or investigation which is being offered to you. You should always ask them more questions if you do not understand or if you want more information.
The information you receive should be about your condition, the alternatives available to you, and whether it carries risks as well as the benefits. What is important is that your consent is genuine or valid. That means:
- you must be able to give your consent
- you must be given enough information to enable you to make a decision
- you must be acting under your own free will and not under the strong influence of another person
Information about you
We collect and use your information to provide you with care and treatment. As part of your care, information about you will be shared between members of a healthcare team, some of whom you may not meet. Your information may also be used to help train staff, to check the quality of our care, to manage and plan the health service, and to help with research. Wherever possible we use anonymous data.
We may pass on relevant information to other health organisations that provide you with care. All information is treated as strictly confidential and is not given to anyone who does not need it. If you have any concerns please ask your doctor, or the person caring for you.
Under the General Data Protection Regulation and the Data Protection Act 2018 we are responsible for maintaining the confidentiality of any information we hold about you. For further information visit the following page: Confidential Information about You.
If you or your carer needs information about your health and wellbeing and about your care and treatment in a different format, such as large print, braille or audio, due to disability, impairment or sensory loss, please advise a member of staff and this can be arranged.