- Reference Number: HEY1160/2023
- Departments: Neonates, Ophthalmology Department, Orthoptic
- Last Updated: 31 December 2023
Introduction
This leaflet has been produced to give you general information. Most of your questions should be answered by this leaflet. It is not intended to replace the discussion between you and the healthcare team, but may act as a starting point for discussion. If after reading it you have any concerns or require further explanation, please discuss this with a member of the healthcare team.
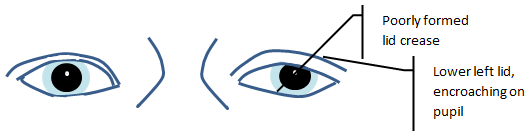
What is Ptosis?
Ptosis is the medical term used for a drooping of the upper eyelid. This can occur in one or both eyes. Ptosis can be congenital (present at birth) or acquired (later in life).
Congenital
Congenital ptosis is most commonly due to a problem with the muscle (levator muscle) that raises the upper eye lid. It is usually noted in early childhood as a droopy/heavy upper eyelid and can vary in appearance. It can be worse if the child is tired or unwell. If one or both upper eyelids are low a child may raise their eye brows or elevate their chin in order to see well. A common type of congenital ptosis is Marcus Gunn ‘jaw winking’ syndrome.
Acquired
Acquired ptosis can occur for a number of reasons including:
- A defect of the tendon which connects the levator muscle to the eyelid. This is usually due to natural ageing changes.
- A weakness in the eyelid muscles, occurring in some rare muscle conditions.
- A problem with the nerve which controls the muscle of the eyelid.
- A mechanical defect caused by anything that increases the weight of the eyelid, such as a cyst or swelling.
Can this impact vision and why do I need to attend appointments?
In the majority of cases ptosis does not affect visual development directly. Children are not born with fully developed vision; in the same way they learn to speak they have to learn to see. If there is a barrier to normal visual development, such as a droopy lid, this can lead to amblyopia (lazy eye).
In children it is advisable to attend orthoptic appointments so that your Orthoptist can ensure that the vision is continuing to develop normally in both eyes. Your Orthoptist may also be able to suggest any adjustments that may make some things easier for your child.
What is the treatment?
Individuals with ptosis often do not require any formal treatment unless there is a risk it will impede visual development. If visual development is affected and there is reduced vision in the affected eye your child may require treatment (amblyopia therapy) in order to encourage visual development in the weaker eye. The orthoptic team will discuss this with you at your appointment.
If the ptosis is covering the pupil or is noticeable, an operation may be considered. Your child will require a general anaesthetic (putting your child to sleep). Surgery is normally performed when a child is old enough to gain his/her co-operation. Often it is advisable to leave surgery as long as possible in order for your child’s facial features to develop, as it may become less noticeable as they get older.
Are there any complications or risks?
Ptosis surgery is complex and it is not possible to guarantee the success of the surgery. The majority of cases are satisfactorily corrected, but it may take more than a single procedure.
Common complications include a lid position that is too high (over-correction), too low (under-correction) or a change in the normal lid margin contour or curve which may become irregular. Sometimes, particularly in congenital ptosis, the lid can fail to look down (lid lag). The droopy lid can also recur at any time in the future and may need further surgery.
Should you require further advice on the issues contained in this leaflet, please do not hesitate to contact the Orthoptic Department on tel: 01482 816605.