
- Reference Number: HEY1639/2026
- Departments: Ophthalmology Department
- Last Updated: 30 April 2026
Introduction
This leaflet has been produced to give you general information about your procedure. Most of your questions should be answered by this leaflet. It is not intended to replace the discussion between you and your doctor but may act as a starting point for discussion. If after reading it you have any concerns or require further explanation, please discuss this with a member of the healthcare team caring for you.
What is a Corneal Graft Transplant?
You have probably been troubled by some symptoms. Following discussion with your doctor they have advised a corneal graft transplant.
A corneal transplant, also called a corneal graft or keratoplasty, is an operation to replace all or part of the cornea with a healthy donor cornea. It may help improve vision, relieve pain or irritation, or treat severe infection or corneal damage.
The type of cornea transplant you have will depend on which part of the cornea is damaged or how much of the cornea needs replacing.
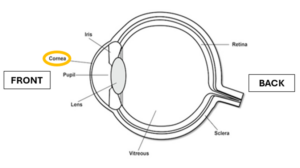
What is the Cornea?
The cornea is the clear dome shaped surface at the front of your eye. It helps focus light so you can see clearly. If it becomes scarred, swollen or losses its clarity, vision becomes blurry or distorted.
Why do I need a Corneal Graft Transplant?
Your doctor may recommend a corneal transplant to:
- Improve vision if the cornea is cloudy or mis-shaped
- Reduce chronic pain or irritation
- Treat severe infection or trauma (e.g. corneal ulcers or perforations)
Alternative treatments may be discussed, such as contact lenses, medications, or partial transplants, depending on your condition.
Types of Corneal Graft Transplant?
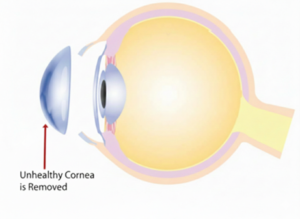
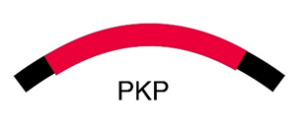
- Full thickness transplant (Penetrating Keratoplasty / PKP)
- Used when the entire cornea is affected
- A circular piece of the damaged cornea is removed and replaced with donor tissue.
- Held in place with fine sutures for up to 12 to 24 months.
- Usually performed under general anaesthesia
- Partial-thickness transplants
Only the affected portion of the cornea is replaced, offering faster recovery and lower risk of some complications, types include:
Front portion:
Superficial Anterior Lamellar Keratoplasty (SALK)
- Only the surface layers of the cornea is replaced, preserving the deeper layers
- Used in cases of surface scarring
- This reduces the risk of rejection and allows for faster healing compared with deeper transplants.
Deep Anterior Lamellar Keratoplasty (DALK)
- Back layer of your cornea remains intact, reducing the risk of rejection and failure.
- May need to convert to full thickness during surgery if required.

Back portion:
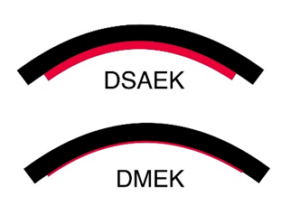
Endothelial Transplants: (DSAEK / DMEK)
For disease affecting only the inner layer
- DSAEK: Back layer & supporting stroma replaced.
- DMEK: Only the thin back layer is replaced.
- Graft is held in place by an air bubble; Post surgery you will need to lie flat on your back for 24 hours till review by surgeon.
- Visual recovery is faster than full-thickness transplants. (6 weeks)
Can there be any complications or risks?
Corneal transplant surgery is generally a safe procedure. However, as with any surgical treatment, there are possible complications and risks that must be considered carefully:
- Infection/inflammation of the eye
- Wound healing problems
- Raised eye pressure (glaucoma) from surgery or steroid drops
- Blurred vision or astigmatism, sometimes needing glasses, contact lenses, or further treatment
- Gradual loss of corneal cells, leading to clouding of the transplant
- Rejection of the transplant, causing redness, pain, light sensitivity, or blurred vision and may require repeat surgery
- Loss of vision
Additional procedure-related risks:
- Full-thickness transplant: higher risk of rejection and wound weakness
- Partial-thickness transplant: rare damage to deeper layers during surgery
- Endothelial transplant: graft movement or detachment, sometimes needing an air reinjection.
Using eye drops as prescribed and attending follow-up visits greatly reduces these risks.
How do I prepare for a Corneal Graft Transplant?
Please read the information leaflet. Share the information it contains with your family (if you wish) so that they can be of help and support. There may be information they need to know, especially if they are taking care of you following this examination.
- Attend pre-assessment clinic as advised.
- Bring a list of current medications; discuss whether to continue them.
- Follow fasting instructions (usually no food 6 hours prior, clear fluids up to 2 hours prior).
- Bring nightwear, slippers, and any aids you need.
- Share information with family who may help with post-op care.
What will happen?
Arrive at the specified time; expect some waiting. The surgeon and ophthalmic team will meet you and discuss your surgery. Surgery usually takes 1 to 2 hours; anaesthesia type depends on your health. Post-op pain is usually mild; analgesia provided if required.
What happens afterwards?
After your operation, your eye will be covered with a protective pad, which is usually removed the next day. Your vision may be blurred, and mild discomfort or swelling is normal. You should use your prescribed antibiotic and steroid drops as directed to prevent infection and rejection. Avoid rubbing your eye and wear an eye shield at night for 2 to 4 weeks. Do not swim, undertake strenuous exercise, heavy lifting, or contact sports until advised it is safe to do so. Protective eyewear is recommended, and you should only drive once your vision meets legal standards and your doctor advises it is safe. If you have had a partial-thickness transplant with an air bubble, you may be asked to lie on your back for several hours after surgery. Stitches are usually non-dissolving and may remain in place for 12 to 24 months; they can be adjusted or removed to help improve vision. You will require regular follow-up appointments, initially frequent and then more spaced out over time, to monitor healing, eye pressure, and signs of rejection or infection. Your eye drops will be gradually reduced as advised by your ophthalmologist.
Possible Complications / When to seek help
When to Seek Help Immediately
- Redness, pain, or watery eye
- Cloudy or foggy vision
- Sensitivity to light
- Trauma to the operated eye
________________________________________
Post-Surgery Recovery
- Vision recovery can take weeks to over a year.
- Glasses or contact lenses may be needed to correct astigmatism.
- Some patients may require secondary surgery for best visual outcomes.
Dos and Don’ts:
- Do take prescribed drops regularly
- Do wear eye protection
- Do rest and avoid strenuous activity
- Don’t rub your eye
- Don’t swim or get water in the eye until cleared
- Don’t drive until advised
Should you require further advice on the issues contained in this leaflet, please do not hesitate to contact the Ophthalmology Department Monday to Friday 08:30AM to 18:00PM on Tel: 01482 608788 / Tel: 01482 816658 or Tel: 01482 604385 if out of hours.
General Advice and Consent
Most of your questions should have been answered by this leaflet, but remember that this is only a starting point for discussion with the healthcare team.
Consent to treatment
Before any doctor, nurse or therapist examines or treats you, they must seek your consent or permission. In order to make a decision, you need to have information from health professionals about the treatment or investigation which is being offered to you. You should always ask them more questions if you do not understand or if you want more information.
The information you receive should be about your condition, the alternatives available to you, and whether it carries risks as well as the benefits. What is important is that your consent is genuine or valid. That means:
- you must be able to give your consent
- you must be given enough information to enable you to make a decision
- you must be acting under your own free will and not under the strong influence of another person
Information about you
We collect and use your information to provide you with care and treatment. As part of your care, information about you will be shared between members of a healthcare team, some of whom you may not meet. Your information may also be used to help train staff, to check the quality of our care, to manage and plan the health service, and to help with research. Wherever possible we use anonymous data.
We may pass on relevant information to other health organisations that provide you with care. All information is treated as strictly confidential and is not given to anyone who does not need it. If you have any concerns please ask your doctor, or the person caring for you.
Under the General Data Protection Regulation and the Data Protection Act 2018 we are responsible for maintaining the confidentiality of any information we hold about you. For further information visit the following page: Confidential Information about You.
If you or your carer needs information about your health and wellbeing and about your care and treatment in a different format, such as large print, braille or audio, due to disability, impairment or sensory loss, please advise a member of staff and this can be arranged.